Cosmetic Eyelid Surgery/ Blepharoplasty Surgery for the Young
Am I too young to have cosmetic eyelid surgery/ blepharoplasty?
Contrary to common belief not all cosmetic eyelid surgery is performed in patients who are 40 years old plus i.e. for rejuvenation purposes.
Around 30% of the cosmetic eyelid surgery performed by Mr Cheung is for patients aged 18-35 ( Mr Cheung does not offer cosmetic surgery to patients under 18 years old).
As with all blepharoplasty surgery, success is often often dependent on careful surgical consultation, planning and meticulous surgery e.g. to create a skin crease which is harmonious with the patient’s facial features, ethnicity and cosmetic wishes.
Although Mr Cheung is happy to consider cosmetic blepharoplasty in patients from the age of 18 years old onwards; as with any cosmetic type procedure, it is vital that the patient is mature enough to consider the potential psychological/ emotional implications as well as the potential risks of any planned surgery.
For this reason, Mr Cheung would therefore normally recommend that patients only consider cosmetic surgery from the age of 25 onwards.
There are various reasons for young patients attending Mr Cheung’s cosmetic clinics but the most common reasons include:
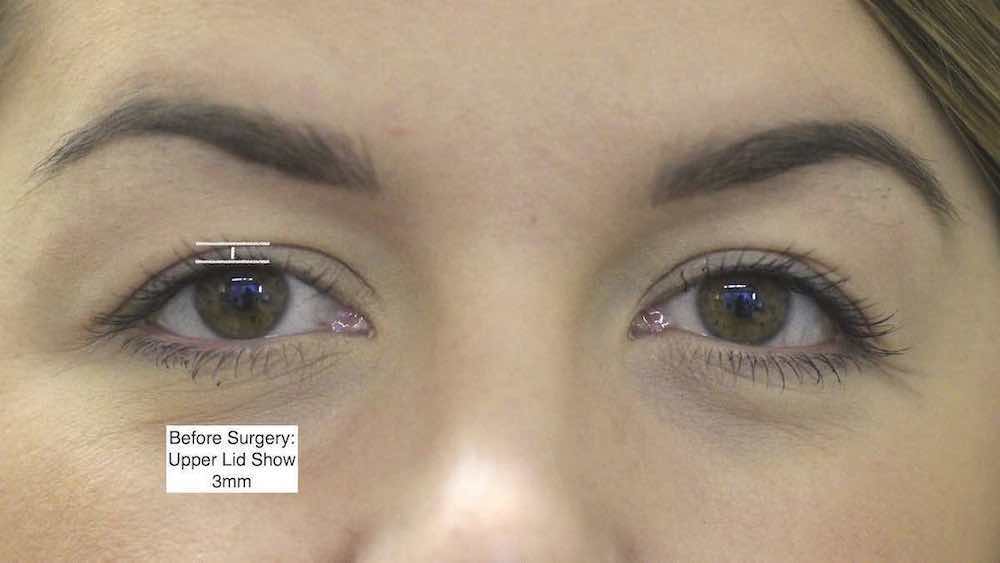
• Young patients wanting greater exposure of their upper eyelids often to enable them to wear eye makeup or to make their upper eyelids look more symmetrical.
• Young patients unhappy with their lower eyelids looking fatty and bulging.
• Young patients feeling that their lower eyelids look tired and hollow.
This sort of cosmetic surgery is therefore designed to alter features which the patient was born with.
Upper Eyelid Anchor Blepharoplasty | Upper Cosmetic Eyelid Surgery in the Young
This sort of surgery is usually only performed by oculoplastic surgeons and involves creating newer, often higher, skin creases to increase the upper lid show (ULS) a.k.a. pretarsal lid show.
• This may involve surgery to both upper eyelids to increase the upper lid show on both sides.
• Whilst for other patients this involves performing surgery to one upper eyelid only to try to improve its symmetry with the eyelid on the other side.
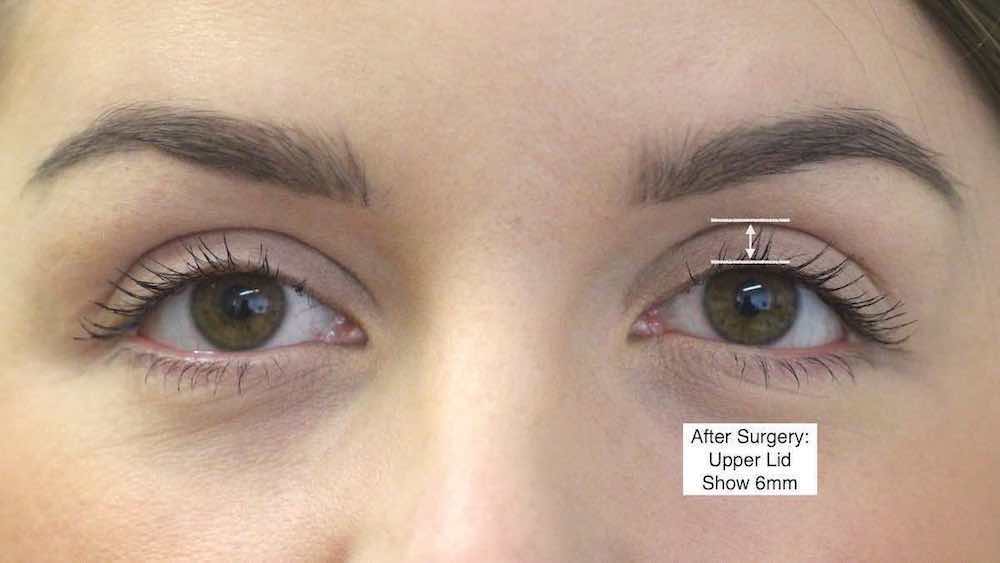
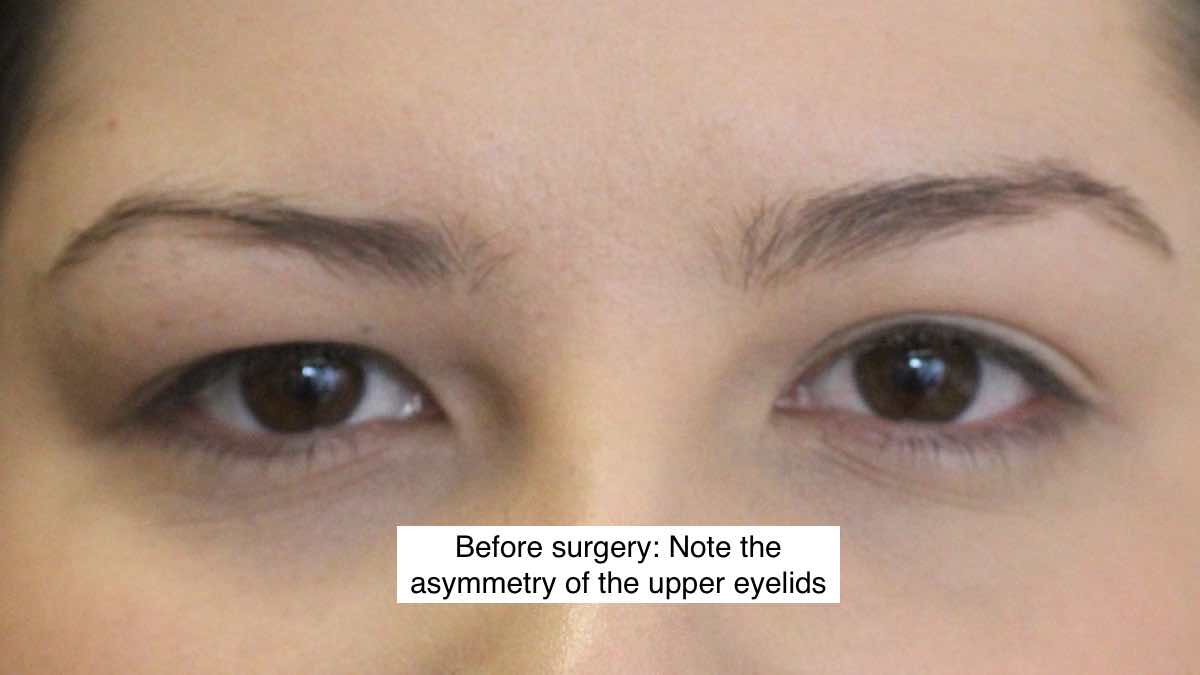
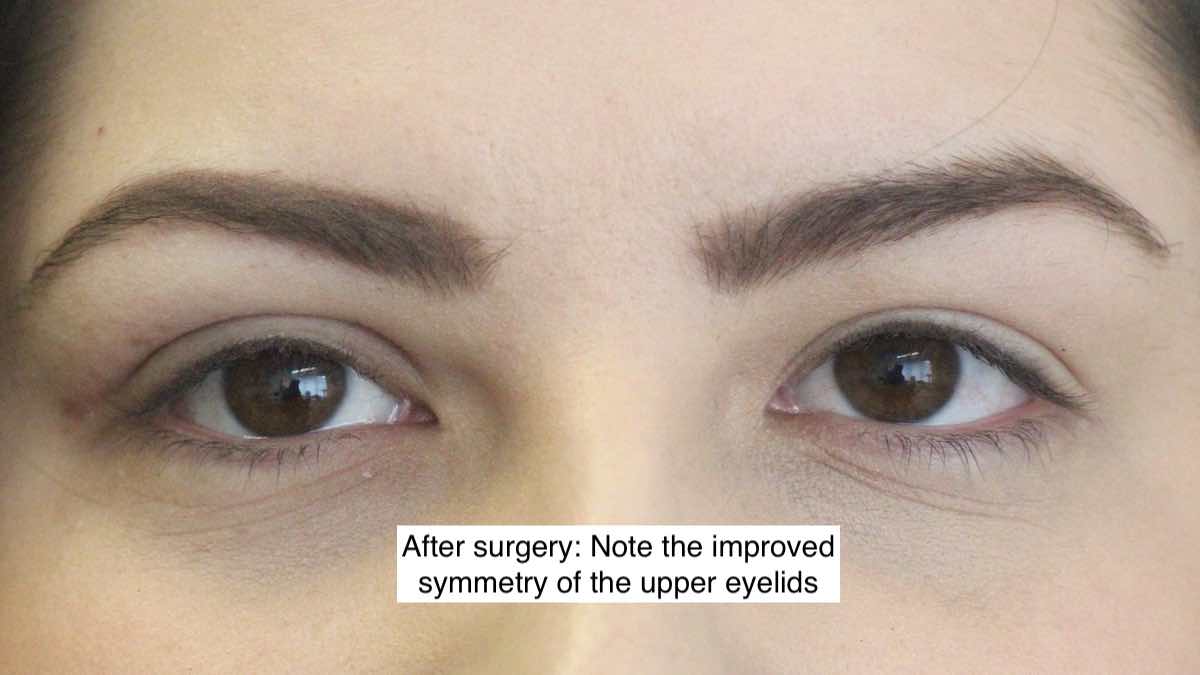
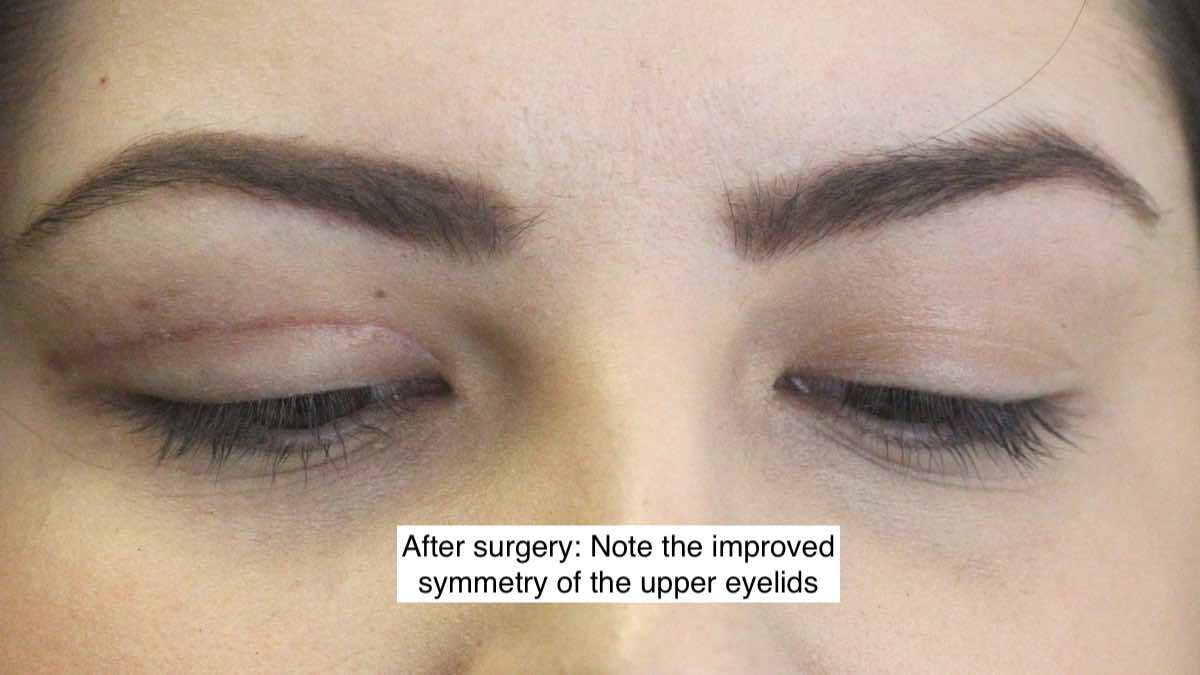
Before and After Pictures of a Young Patient After Anchor Blepharoplasty Surgery To Both Upper Eyelids
- This 23 year old lady had always desired greater exposure of the eyelid to enable her to wear eye shadow.
- One can see that she has poorly defined skin creases before surgery. Surgery was performed under local anaesthetic to create a new higher more defined skin creases.
- This is very specialised surgery performed only by oculoplastic surgeons.
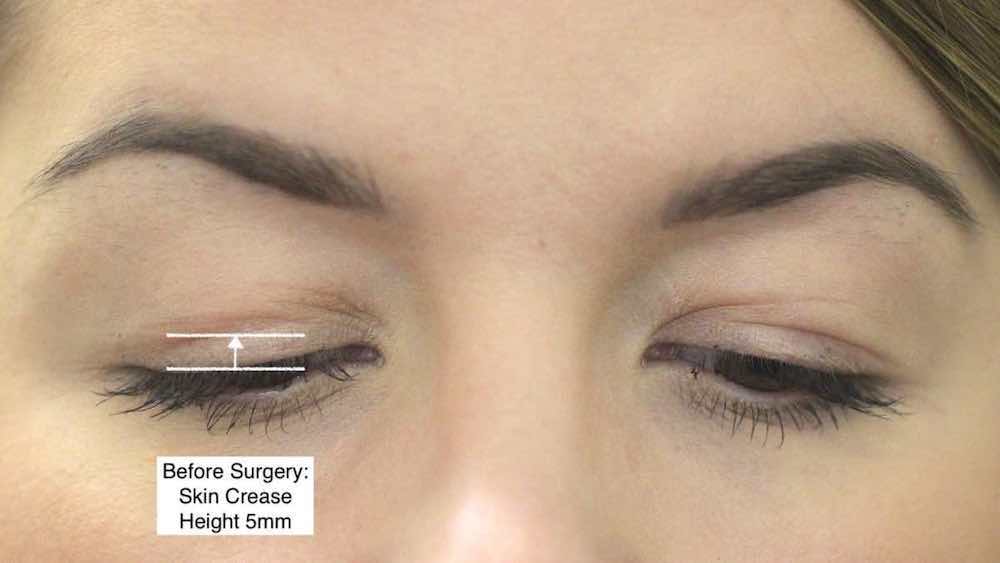
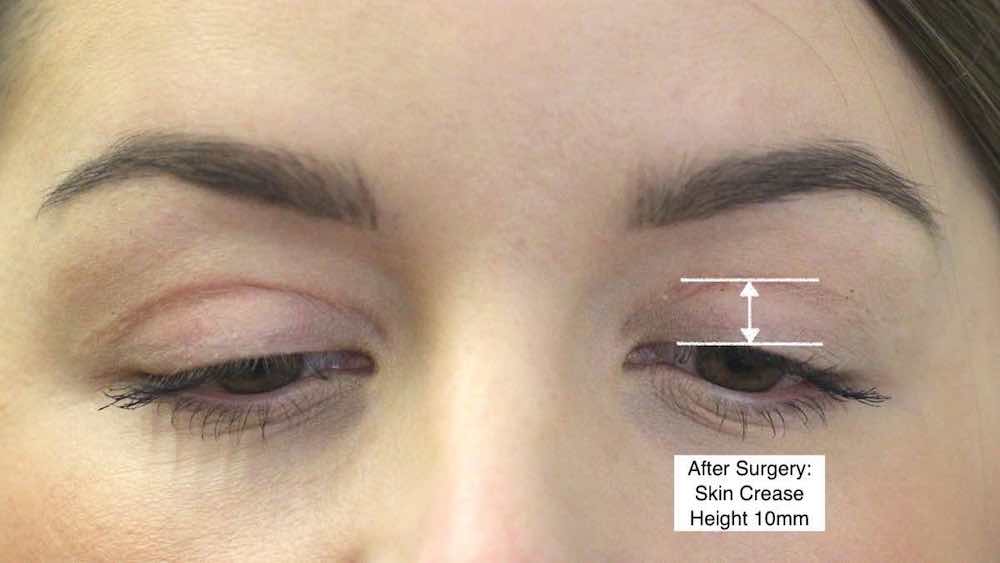
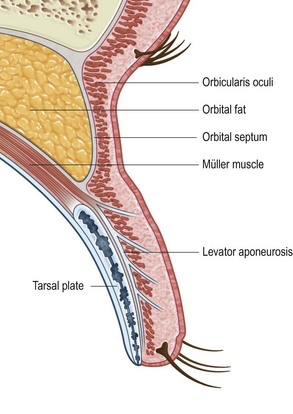
The normal skin crease is formed due to the presence of an attachment between the skin and the fibres of the levator aponeurosis (main tendon responsible for elevating the upper eyelid). An anchor blepharoplasty is a specialised type of blepharoplasty which involves creating a new higher skin crease by making a incision where you want the new skin crease to be, carefully exposing the levator aponeurosis and then creating a new attachment between the skin and the levator aponeurosis by suturing the skin to the levator aponeurosis with so called anchor sutures (hence name).
Unlike older patients, young patients often do not have much excess skin to remove within the eyelid fold as one would normally do for a conventional upper eyelid blepharoplasty. Therefore to increase upper lid show safely, one cannot simply just remove skin as doing so would cause closure problems of the eyelid leading potentially to a dry eye syndrome.
By elevating the skin crease however, one can therefore increase the upper lid show safely. This sort of surgery evolved Mr Cheung’s work from incisional Oriental blepharoplasty where that sort of surgery in essence is all to do ablation of unwanted skin creases and then formation of new skin creases to the patient’s request.
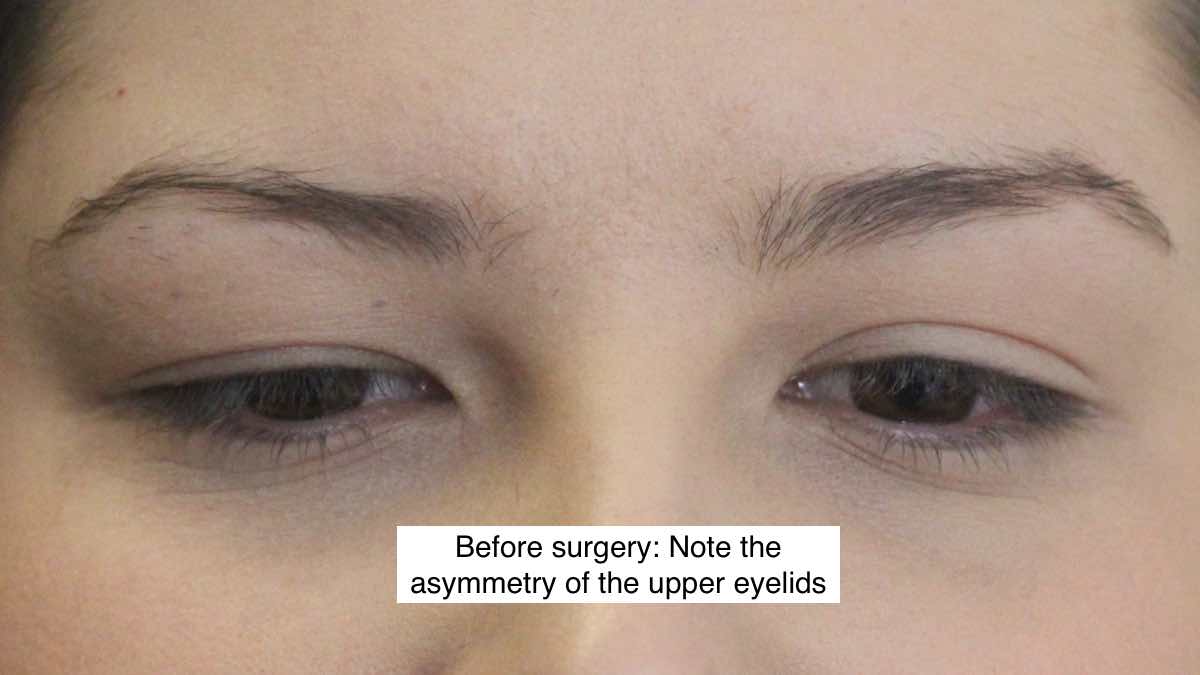
Before and Six Weeks After Pictures of a Young Patient After Anchor Blepharoplasty Surgery To HER Right Upper Eyelid
- This young lady was born with marked asymmetry of her upper eyelids.
- Note the upper lid show was much less on HER right upper lid due to her having a lower skin crease. She underwent surgery to HER right upper eyelid to match the other side.
- The right upper eyelid is still minimally swollen at 6 weeks.
Lower Cosmetic Eyelid Surgery in the Young
For most young patients attending Mr Cheung's clinics for their lower lids, their main complaint is typically of them looking either too bulging (lower lid fat bags) or slightly too hollow (tear trough deformity).
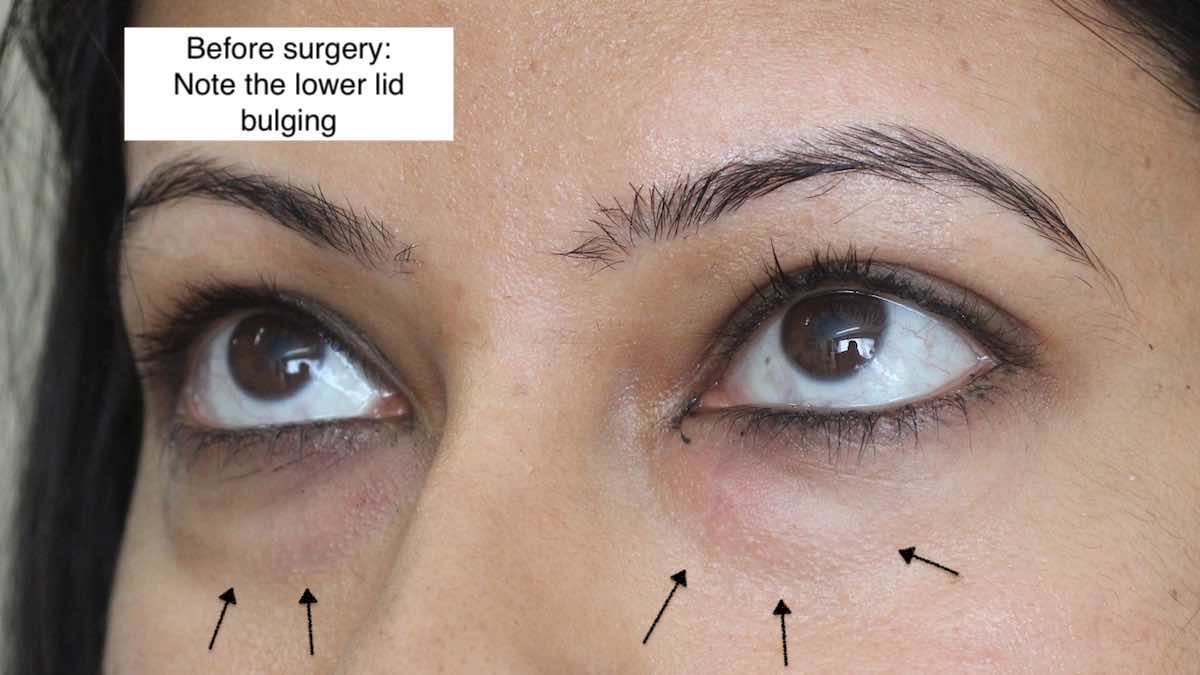
Before and One Week After Pictures of a Young Patient After Lower Transconjunctival Lower Lid Blepharoplasty
- As the skin and muscle quality is usually excellent in young patients, these do not require treatment. Mr Cheung has therefore performed a transconjunctival lower lid blepharoplasty where the access incision is made on the back surface of the lower eyelids, thus avoiding the the need for a skin incision or risk getting a scar.
- This young lady complained of bulging of the lower lid before surgery.
- Surgery is typically performed under sedation and a small amount of fat is removed from the fat pockets to make them look less apparent. Recovery time is very quick and most patients are back to work after 2 weeks.

Tear trough filler treatment in the young to correct lower eyelid hollows/ dark circles
For most young patients though with hollow looking lower eyelids, surgery is NOT required. Instead these patients often do very well without surgery using tear trough filler injections of restylane
-

Tear trough deformity in a 30 year old lady. She complained that she looked tired. -

Notice that she has some hollowing under her eyes (tear trough deformity) and a mild bulging of a fat bag -

She complained that she had looked tired even in her teens and that this had worsened as she got older. -

Immediately following injection of Restylane. Only a tiny volume was necessary on each side -

Notice the single injection points when using a microcannula technique -

There was minimal bruising and the patient can return to work the following day -

Two weeks Restylane injection for tear trough deformity. -

All the bruising has disappeared. The Restylane filler not only fills up the under eye hollowing but also helps disguise the mild bulging from the small fat bag -

Before treatment again
-

After treatment again
How is blepharoplasty/ cosmetic eyelid surgery performed?
- default_titlePrior to any surgery, the surgeon should discuss with you what you wish to achieve, what is safely achievable and the risks and benefits of surgery. At the end of the consultation, the surgeon should be able to develop a surgical plan for that particular patient. Each patient is an individual, and the surgical plan reflects this.
- default_titlePrior to any eyelid operation, it is highly recommended that every patient should ideally undergo a formal eye examination either by the surgeon who is going to be performing the procedure or an impartial ophthalmologist.
- default_titleBlepharoplasty/ eyelid cosmetic surgery is performed commonly as a day case procedure.
- default_titleMuch like the word ‘haircut’, the term blepharoplasty describes refashioning of the eyelid in general. The procedure itself will have slight variations depending on the patient. Because oculoplastic surgeons perform more eyelid operations than any other type of surgeon, they are more equipped to offer the full repertoire of techniques to address different variations in patient anatomy.
- default_titleLike all types of eyelid surgery, blepharoplasty surgery, either for cosmetic or functional reasons, can be performed under local anaesthesia, local anaesthesia with mild sedation, or general anaesthesia.
- Show More
Upper Eyelids
- default_titleFor upper eyelid blepharoplasty, the surgeons will draw some lines on the upper eyelid.
- default_title Surgery can be performed using either general anaesthetic or local anaesthetic. The vast majority of patients opt for local anaesthesia since its is quicker and very acceptable. Sometimes the anaesthetist may administer some sedation through a vein in the back of the hand to make relax the patient further.
- default_title Removal of the excess skin is then performed using either a scalpel, carbon dioxide laser, or radiofrequency cutting device. The incisions are situated within the normal skin crease of the eyelid so that afterwards, the incision scar is hidden and becomes invisible.
- default_titleFor those patients with bulging fat in the upper eyelid, the fat is then either sculpted away or repositioned.
- default_titleAn oculoplastic surgeon can then perform any additional procedures as necessary , for example, correcting a droopy eyelid with eyelid ptosis surgery, repositioning a prolapsed tear gland, debulking of any prolapsing orbital fat or lifting/ stabilising the eyebrow position.
- default_titleThe wound is then closed with sutures. Although their removal is required, non-dissolvable sutures are sometimes used, because of their more predictable cosmetic result. In an anchor blepharoplasty, an attachment is created using stitches between the skin incision and the main tendon within the eyelid (levator aponeurosis) thus creating a skin crease.
- Show More
-

-

2 weeks following surgery
-

After Upper and Lower Blepharoplasty: The patient remarked how her friends were amazed with the subtle natural improvement
Lower Eyelids
- default_titleFor patients excess skin causing wrinkles, the incision can be made in the skin just below the eyelash line so that the excess skin can be removed after the excess fat is addressed first. The incision is so close to the eyelash line that it becomes invisible within a few weeks of surgery. If there are eye bags ( which is usually caused by the normal orbital fat prolapsing forwards) this can be addressed at the same time through the same incision.
- default_titleIn those patients where skin redundancy is not an issue and the only problem is eyelid bags due to bulging orbital fat, the incision can be made along the inside of the lower eyelid (transconjunctival approach) and the fat prolapse can be addressed resulting in sutureless scarless surgery. This results in a much quicker recovery time following surgery.
- default_titleThere are various ways of addressing prolapsing fat in the lower eyelid and a good cosmetic surgeon should be able to discuss with you the most appropriate options. These include simple fat removal (debulking) to repositioning. In patients with a tear trough deformity, a popular technique which has gained popularity recently is to drape this fat over the edge of the socket and use it to replace the fat which has started to disappear on the rim of the orbit itself. Therefore, instead of simply disposing of the orbital fat, the surgeon is utilising it as a filler.
- default_titleLower eyelid blepharoplasty is technically more challenging than upper eyelid blepharoplasty due to its slimmer margin for error and riskier potential complications. For this reason, many surgeons choose only only concentrate on upper eyelid blepharoplasty.
- default_titleThe surgery performed will be individual to that patient. For example, eyelid tendons may need to be tightened, the bulging fat may be excised or redistributed, the midface/cheek may be lifted, some of the wrinkles may be removed, the hollows underneath the eyelids may be softened and filled. A good cosmetic surgeon should be able to discuss with the patient a personalised surgical plan: customised to the patient's anatomy, the patient's wishes and expectations.
- Show More
Frequently Asked Questions
It is often advisable to have someone accompany you on the day of surgery, particularly if the surgery is performed as a day case procedure. Rarely, the eyes may be covered with pressure dressings for an hour, to help reduce the build up of any postoperative swelling. As the anaesthetic wears off, your eyelids may feel tight and sore, but this wears off quickly and is usually easily treated with simple painkillers. If the postoperative pain is severe, this may indicate a serious problem and patients should get in touch with their surgeon immediately.
You will advised to sleep upright and apply regular cold compresses to the eyelids to reduce the postoperative swelling. It is especially important to keep your wounds clean and dry. Eye drops are commonly provided to help soothe the eyes which can feel slightly dry due to temporary impairment of the normal blink reflex following surgery.
-Swelling and minor bruising is normal and peaks about 24-48 hours after the procedure.
-However 90% of the swelling usually disappears by 10 days but minor swelling may still persist for 10-12 weeks depending on the complexity of the procedure. For example, most of Mr Cheung's patients who return to work after 10-14 days often comment that their work colleagues remark that they look fresher but often do not realise that any surgery has been performed.
-Most patients return back to work about 10-14 days after blepharoplasty surgery.
- The first clinic visit following surgery is usually scheduled for 1 - 2 weeks following surgery. Mr Cheung often personally removes any skin sutures with the aid of an examination microscope to ensure there is no retention of the fine skin stitches.
-Make up can be safely used usually from the 10th postoperative day.
- Most patients are usually discharged at 3-6 months following surgery.
As with any cosmetic procedure, the patient's part in expecting a realistic outcome and understanding the potential complications is probably more important than the skill of the surgeon. Any good surgeon will take the time to chat with the patient so that they have a good understanding of what to expect and what is realistically achievable. Patients with unrealistic expectations are likely to be disappointed no matter how skilled the surgeon or good the postoperative result.
Complications are extremely rare and the vast majority of patients are extremely satisfied following surgery. The complications of blepharoplasty surgery include:
- default_titleEyelid Asymmetry: where one side does not match the other
- default_titleUndercorrection where insufficient skin/ orbital fat has been removed. It is important to be realistic about how much skin can safely be removed.
- default_titleOvercorrection-If too much skin is removed during upper eyelid blepharoplasty, the eyelid may not be able to close properly (termed lagophthalmos), which can be sight threatening. Lagophthalmos can be temporary from eyelid swelling, or permanent if too much skin from the upper eyelid was removed. The cornea (clear window on the front of the eye) may start to dry out due to the incomplete closure of the eyelid. This may be sight threatening since the cornea may ulcerate as a result. For severe cases of lagophthalmos, a skin graft or flap to replace the upper eyelid skin shortage may be necessary to allow the eyelid to function normally again.
- default_titleTemporary dry eye commonly occurs following upper eyelid blepharoplasty surgery and is commonly due to temporary impairment of the muscles involved in eyelid closure. Ocular lubricant drops are commonly prescribed for a few weeks following surgery for symptomatic relief. Less commonly though, permanent dry eye may result particularly particularly following excessive skin removal (both in upper and lower eyelid blepharoplasty) and in patients who have pre-existing problems with dry eye, tear film problems, previous refractive surgery and ocular surface problems. It is for this reason that the Dept of Health recommends that all patients undergoing any type of blepharoplasty surgery undergo a formal assessment by an ophthalmologist including testing ocular motility, tear film production and quality assessment.
- default_titleIf too much lower eyelid skin is removed, the eyelid may look hollowed out, too concave or may cause the eyelid to turn outwards leading to ectropion formation. All oculoplastic surgeons are trained to avoid this by performing additional procedures if necessary e.g. eyelid tendon tightening such as lateral canthopexy.
- default_titleScarring can also occur post-operatively, leading to a poor cosmetic outcome. Scarring following lower eyelid blepharoplasty can result in the lower eyelid being pulled out and downwards, leading to an unnatural appearance and ectropion. Corrective surgery may be necessary to address this. It can usually be avoided by meticulous dissection in the correct surgical planes and is rare in the hands of oculoplastic surgeons.
- default_titleAcute glaucoma is an rare but potentially blinding complication that can occur with any type of eyelid surgery and occurs when the internal pressure of the eye starts to rise as a result of some of the side effects of some of the drugs and injections utilised during eyelid surgery. Oculoplastic surgeons are trained to recognise and manage this complication through their general ophthalmology training. It is recommended in the US, that a formal ophthalmological assessment be performed prior to eyelid surgery to look for the potential risk factors for this complication.
- default_titleBleeding into the skin, known as a skin haematoma, after the procedure is an uncommon complication and excessive bruising leading to a collection of blood within the tissue. It is critical to stop all tablets which may increase the risk of bleeding and your surgeon should advise you about this prior to surgery. In the first few days following surgery, you should avoid any vigourous activity such as lifting, bending, since this can worsen any bruising or swelling of the eyelids.
- default_titleCorneal abrasion is when the corneal surface is damaged either due to the inadvertent trauma. This complication is extremely rare in the hands of oculoplastic surgeons.
- default_titleEyelid ptosis- Uncommonly the main tendon (levator aponeurosis) within the eyelid may be damaged during cosmetic eyelid surgery causing the actual eyelid itself to descend and stay permanently low. This complication is extremely rare for oculoplastic surgeons since they routinely operate on this structure anyway and the most experienced in recognising the complex anatomy. Indeed, oculoplastic surgeons routinely perform ptosis surgery anyway and may recommend simultaneous ptosis correction/ repair in patients who already have a compromised eyelid tendon.
- default_titleSunken eye (enophthalmos) and hollow eyelids- The fat within the socket (orbital fat) normally starts to shrink with age leading the the eyeball looking sunken over time. However, an artificially sunken eye can occur following excessive orbital fat removal. Similarly if excessive fat is removed the eyelids can look artificially hollow (sometimes known as skeletonisation). This complication occurs less commonly now surgeons have learnt to avoid it by being very conservative with orbital fat removal and performing safer techniques e.g. orbital fat repositioning.
- default_titleBy far, the worst complication of blepharoplasty and thankfully the rarest, is an orbital haematoma. Uncontrolled bleeding, usually from a blood vessel from manipulation of some of the pockets of fat, results in compression on the optic nerve and its blood supply. If left untreated, permanent blindness can occur. Early diagnosis—recognised by severe eye pain or visual changes—is critical. Urgent reoperation may be necessary to stem the bleeding point and relieve the pressure on the optic nerve. It is for this reason, that eyelid plastic operations should ideally be performed by surgeons who are experienced in handling the fat of the eye socket to not only avoid this problem but also be able to manage it quickly and safely should it arise. Oculoplastic surgeons perform more operations within the orbit and around the eyelids than any other type of surgeon and are therefore best equipped to avoid and manage this rare but fearsome complication.
- Show More
It is for all these reasons that Mr Cheung tends to err on the side of caution i.e. towards conservative blepharoplasty surgery to reduce the risk of complications and also give a more harmonious balance appearance, to try and avoid a 'plastic' unnatural look. Most complications can be avoid with careful preoperative examination, surgical planning and meticulous operative technique.
Yes you can have blepharoplasty surgery for functional reasons on the NHS i.e. if your eyelid hooding is so severe that it interferes with your visual field or if is for rehabilitation purposes from some pathological process e.g. for thyroid eye disease.
However the NHS is unlikely to fund blepharoplasty surgery purely for cosmetic purposes for the sake of rejuvenation purposes e.g. severe thyroid eye disease, amyloidosis.
For quite some time now, most CCGs (clinical commissioning groups) have brought out their eligibility criteria which patients would have to meet prior their surgery being agreed to be funded by their local NHS.
Dudley Procedures of Limited Clinical Value/ Aesthetic Policy Document 2019
Sandwell and West Birmingham/ Birmingham and Solihull CCG Policy for Cosmetic Surgery - Eyelid Surgery 2019
