Facial Nerve Palsy & Bell's Palsy
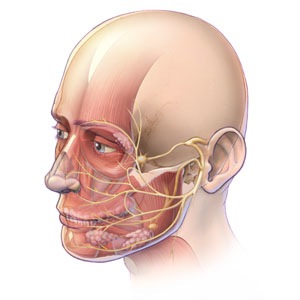
The facial nerve is a complex nerve which originates from the brainstem (junction between the brain and spinal cord), exiting the skull by going through the middle ear and then goes on to supply most of the muscles of facial expression.
The term Bell’s palsy describes a sudden weakness of the facial muscles due to paralysis of facial nerve. Gradual resolution occurs in the vast majority of cases. Although its cause has never been found, various causes have been suspected including viral infection or a mini-stroke like event.
Facial nerve palsy is a wider term describing weakness of the face due to loss of function of the facial nerve. The causes of facial nerve palsy are therefore many and include tumours, strokes, infections, trauma, surgery but the vast majority of facial nerve palsies are sudden, self resolving and without apparent cause i.e. Bell’s palsy.
Bell’s palsy is:
- Relatively uncommon with 10-30 cases per 100000
- Commoner in diabetics, pregnancy and in immunocompromised patients.
- Thought to affect 2 age groups of patients (20-40 years old and 70-80 years old)

Clinical Features of Facial Nerve Palsy / Bells Palsy
- Weakness of the facial muscles
- Problems closing the eye which can lead to watering of the eye, painful irritation of the eye and visual blurring.
Problems which can arise include:
-Lagophthalmos - the inability to close the eye due to paralysis of the upper eyelid
-Ectropion- an out-turning eyelid due to paralysis of the lower eyelid
-Corneal exposure - the corneal surface may start to ulcerate due to poor wetting
-Brow ptosis - drooping of the eyebrow due to paralysis of the forehead muscles
-Midface/Cheek ptosis - a drooping descended cheek due to paralysis of the cheek muscles
-Abnormal spasms of the muscles due to abnormal healing of the damaged nerve
-Crocodile tears- tearing of the eye due to excess tear production associated with chewing
-

Bells palsy: 2 weeks after onset. Notice the patient's difficulty in trying to close his right eye in the early stages of the palsy (the eyelid shows 10mm of non-closure).
-

Bells palsy: 6 weeks later: Although his eyelid closure has improved dramatically 6 weeks later, the patient still complains of a sore right eye since the eyelid still closes incompletely and shows 5mm of non-closure
Treatment of Facial Nerve Palsy and Bells Palsy
1. Ensure correct diagnosis
2. Supportive treatment whilst awaiting self resolution.
3. Facial rehabilitation for longstanding changes.
Ensure correct diagnosis
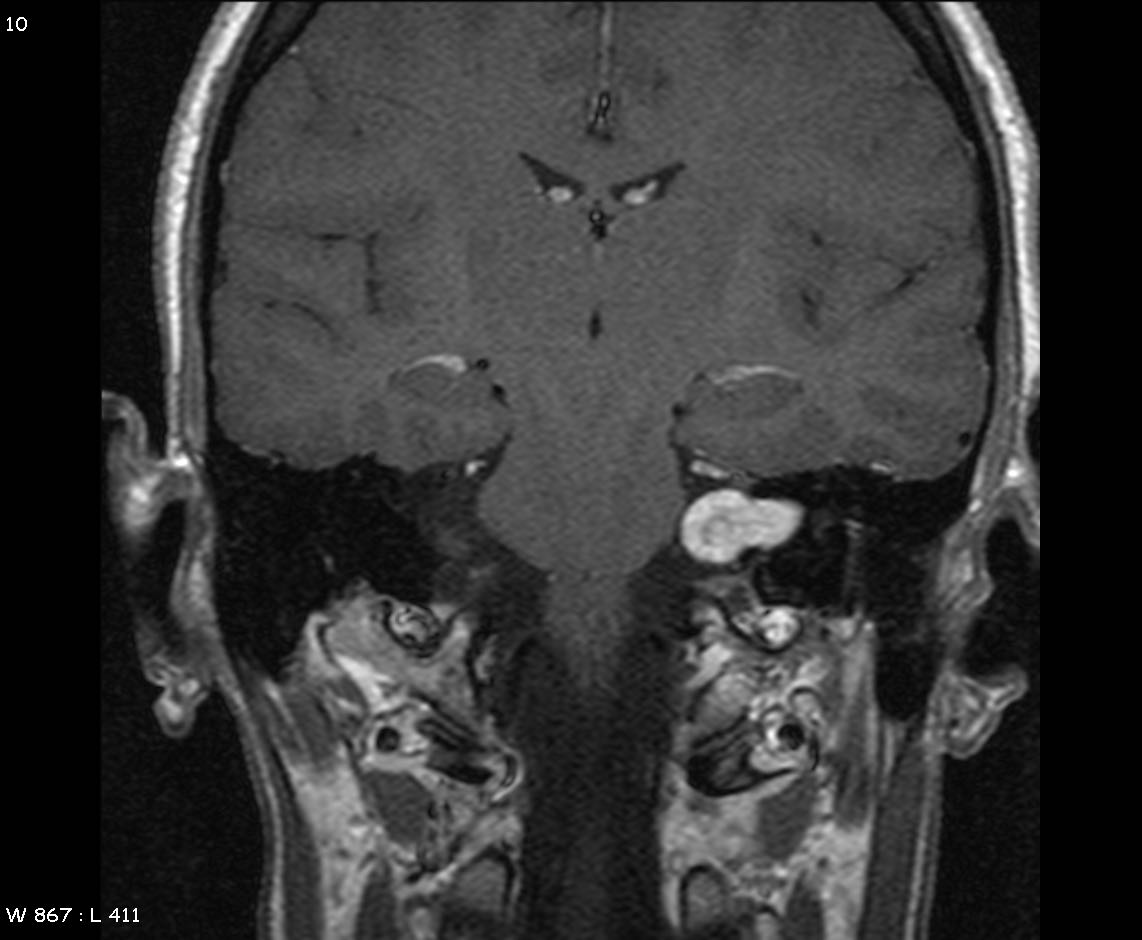
This is to rule out a more sinister cause other than Bell’s palsy causing the facial nerve palsy. This will involve careful examination, history taking and sometimes specialised scans of the brain. Because most Bell’s palsy show signs of resolution within 6-8 weeks, any facial nerve palsy which does not show any signs of improvement usually warrants either CT or MRI scans of the brain. Some clinicians feel that the diagnosis of Bell's palsy (where there is no apparent cause) can only be made after all other causes are ruled out first.
Early Supportive Treatment Whilst Waiting for Self Resolution
It is very important that any patient with a facial nerve palsy be reviewed by an ophthalmologist (preferably with an oculoplastic interest) to assess the risk of development eye surface problems due to the weakness of the blink reflex. He/ she will be able to classify whether a patient's facial nerve palsy is at risk of causing corneal problems:
Low Risk Facial Nerve Palsy: Many patients complain of a sore watering eye due to dryness of the cornea from improper wetting. This is either because of failure of the eye to close (lagophthalmos) or a reduction of the normal blink reflex on the affected side. Therefore eye drops and ointments are often helpful and give symptomatic relief.
Moderate Risk Facial Nerve Palsy: in some patients the lagophthalmos (inability to close the eye) may be particularly severe. In these patients, the cornea (clear window of the front of the eye), is at risk of drying out, ulcerating with possible perforation of the eye itself. For patients with these high risk eyes, their doctors may also recommend that in addition to the use of sticky ointments and drops to help lubricate the eye; other techniques may also be required e.g. taping the upper eyelid down to the cheek, sticking a small external eyelid weight on to the skin of the eyelid to aid closure, wearing cling film to cover the eye at night, wearing moisture goggles at night, botulinum toxin injections to the eyelid (to cause it to droop).
High Risk Facial Nerve Palsy: In the small proportion of patients where the facial nerve dysfunction is particularly severe and the eye is starting to suffer despite maximal conservative measures, urgent surgery may be necessary to protect the eye whilst awaiting self improvement.
Rehabilitation for Longstanding Incomplete Recovery
The vast majority of patients with facial nerve palsy, especially the Bell’s Palsy type, go on to make a complete recovery. However a small proportion of patients will continue to have long term functional and/or cosmetic problems e.g. watering eyes, drooping brows and cheeks, sore red eye due to lagophthalmos.
Facial Spasms
A small minority of patients can develop abnormal involuntary twitches, tics or spasms of the facial muscles following facial nerve palsy. Different patterns of twitching can develop e.g. blepharospasm, hemifacial spasm.
Botulinum Toxin (Botox, Dysport) injections are often very helpful in paralysing the affected twitching muscles. These injections although temporary, requiring repeat injection (usually every 3-6 months), are often very well tolerated providing welcome symptomatic relief.
Surgical Rehabilitation
Oculoplastic surgeons such as Mr Cheung offer different many types of operations to help the rehabilitation of patients with facial nerve palsy. Each patient needs to be treated on an individual basis. Different patients with facial nerve palsy will have different clinical features with varying severity of problems.
Facial Nerve Palsy Gallery
-

Typical features of long term facial nerve palsy on the patient's left. Note drooping brow and forehead.
-

Direct Brow Lifting: Preoperative marking of the amount of skin removal required to lift up the droopy eyelid
-

1 week following surgery. Note the symmetry of the eyebrows
-

3 months following surgery. Note the scars have started to fade away to look lke normal forehead wrinkle lines.
-

Facial Nerve Palsy: This patient cannot close his left eye
-

Facial Nerve Palsy: This patient cannot close his left eye
-

2 months following insertion of a gold weight into the eyelid. This aids closure of the eye. Notice the mild swelling in his left upper eyelid. This is the gold weight which sits below the skin.
-

This weight is perfectly sized for the patient- aiding closure of the eye without causing a droopy eyelid